| Drug Name |
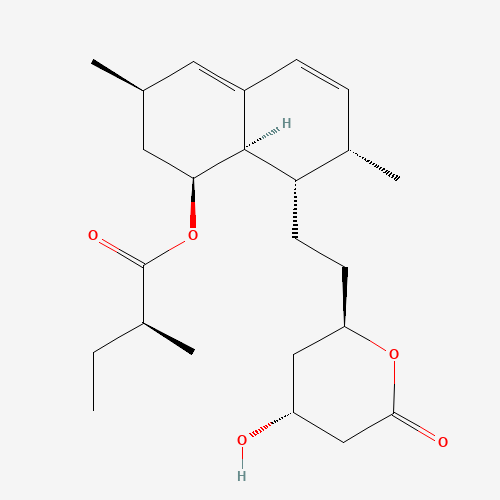
Lovastatin |
| Drug ID |
BADD_D01325 |
| Description |
Lovastatin, also known as the brand name product Mevacor, is a lipid-lowering drug and fungal metabolite derived synthetically from a fermentation product of _Aspergillus terreus_.[A174550] Originally named Mevinolin, lovastatin belongs to the statin class of medications, which are used to lower the risk of cardiovascular disease and manage abnormal lipid levels by inhibiting the endogenous production of cholesterol in the liver.[A174553] More specifically, statin medications competitively inhibit the enzyme hydroxymethylglutaryl-coenzyme A (HMG-CoA) Reductase,[A181421] which catalyzes the conversion of HMG-CoA to mevalonic acid and is the third step in a sequence of metabolic reactions involved in the production of several compounds involved in lipid metabolism and transport including cholesterol, low-density lipoprotein (LDL) (sometimes referred to as "bad cholesterol"), and very low-density lipoprotein (VLDL). Prescribing of statin medications is considered standard practice following any cardiovascular events and for people with a moderate to high risk of development of CVD, such as those with Type 2 Diabetes. The clear evidence of the benefit of statin use coupled with very minimal side effects or long term effects has resulted in this class becoming one of the most widely prescribed medications in North America.[A181087, A181406]
Lovastatin and other drugs from the statin class of medications including [atorvastatin], [pravastatin], [rosuvastatin], [fluvastatin], and [simvastatin] are considered first-line options for the treatment of dyslipidemia.[A181087, A181406] Increasing use of the statin class of drugs is largely due to the fact that cardiovascular disease (CVD), which includes heart attack, atherosclerosis, angina, peripheral artery disease, and stroke, has become a leading cause of death in high-income countries and a major cause of morbidity around the world.[A181084] Elevated cholesterol levels, and in particular, elevated low-density lipoprotein (LDL) levels, are an important risk factor for the development of CVD.[A181087,A181553] Use of statins to target and reduce LDL levels has been shown in a number of landmark studies to significantly reduce the risk of development of CVD and all-cause mortality.[A181090,A181093,A181096,A181427,A181475,A181538] Statins are considered a cost-effective treatment option for CVD due to their evidence of reducing all-cause mortality including fatal and non-fatal CVD as well as the need for surgical revascularization or angioplasty following a heart attack.[A181087, A181406] Evidence has shown that even for low-risk individuals (with <10% risk of a major vascular event occurring within 5 years) statins cause a 20%-22% relative reduction in major cardiovascular events (heart attack, stroke, coronary revascularization, and coronary death) for every 1 mmol/L reduction in LDL without any significant side effects or risks.[A181397, A181403]
While all statin medications are considered equally effective from a clinical standpoint, [rosuvastatin] is considered the most potent; doses of 10 to 40mg [rosuvastatin] per day were found in clinical studies to result in a 45.8% to 54.6% decrease in LDL cholesterol levels, while lovastatin has been found to have an average decrease in LDL-C of 25-40%.[A174580,A181409,A181535,A181538,A1793] Potency is thought to correlate to tissue permeability as the more lipophilic statins such as lovastatin are thought to enter endothelial cells by passive diffusion, as opposed to hydrophilic statins such as [pravastatin] and [rosuvastatin] which are taken up into hepatocytes through OATP1B1 (organic anion transporter protein 1B1)-mediated transport.[A181424,A181460] Despite these differences in potency, several trials have demonstrated only minimal differences in terms of clinical outcomes between statins.[A181438, A181427] |
| Indications and Usage |
Lovastatin is indicated to reduce the risk of myocardial infarction, unstable angina, and the need for coronary revascularization procedures in individuals without symptomatic cardiovascular disease, average to moderately elevated total-C and LDL-C, and below average HDL-C. It is indicated as an intervention alternative in individuals presenting dyslipidemia at risk of developing atherosclerotic vascular disease. The administration of this agent should be accompanied by the implementation of a fat and cholesterol-restricted diet.[F4661]
Therapy with lipid-altering agents should be a component of multiple risk factor intervention in those individuals at significantly increased risk for atherosclerotic vascular disease due to hypercholesterolemia. Lovastatin is indicated as an adjunct to diet for the reduction of elevated total-C and LDL-C levels in patients with primary hypercholesterolemia (Types IIa and IIb2), when the response to diet restricted in saturated fat and cholesterol and to other nonpharmacological measures alone has been inadequate.[F4661,F4664]
Lovastatin is also indicated to slow the progression of coronary atherosclerosis in patients with coronary heart disease as part of a treatment strategy to lower total-C and LDL-C to target levels.[F4661]
Lovastatin is indicated as an adjunct to diet to reduce total-C, LDL-C and apolipoprotein B levels in adolescent boys and girls with Heterozygous Familial Hypercholesterolemia (HeFH) who are at least one year post-menarche, 10 to 17 years of age, with HeFH if after an adequate trial of diet therapy the following findings are present: LDL-C remains greater than 189 mg/dL or LDL-C remains greater than 160 mg/dL and there is a positive family history of premature cardiovascular disease or two or more other CVD risk factors are present in the adolescent patient.
Before administering lovastatin, it is important to rule out the presence of secondary causes of hypercholesterolemia and a lipid profile should be performed.
Prescribing of statin medications is considered standard practice following any cardiovascular events and for people with a moderate to high risk of development of CVD. Statin-indicated conditions include diabetes mellitus, clinical atherosclerosis (including myocardial infarction, acute coronary syndromes, stable angina, documented coronary artery disease, stroke, trans ischemic attack (TIA), documented carotid disease, peripheral artery disease, and claudication), abdominal aortic aneurysm, chronic kidney disease, and severely elevated LDL-C levels.[A181087, A181406] |
| Marketing Status |
approved; investigational |
| ATC Code |
C10AA02 |
| DrugBank ID |
DB00227
|
| KEGG ID |
D00359
|
| MeSH ID |
D008148
|
| PubChem ID |
53232
|
| TTD Drug ID |
D06WTZ
|
| NDC Product Code |
50090-3881; 51407-251; 63187-194; 68788-9667; 0615-8152; 0093-0928; 43063-493; 43063-548; 43063-939; 43353-995; 50090-0762; 51655-469; 51655-873; 53002-1385; 53002-5701; 55289-881; 61442-141; 63629-3583; 68071-2653; 68071-3127; 70518-0113; 71205-440; 71335-1633; 50090-0759; 51655-558; 63187-345; 66267-506; 68001-315; 68788-8232; 70515-629; 61919-547; 63187-814; 63629-1191; 68645-567; 68788-7056; 71205-199; 51846-1014; 43063-692; 50090-0757; 61919-941; 63629-1018; 63629-1178; 68180-468; 68180-469; 70515-628; 71205-992; 71335-0045; 0615-8151; 50090-3396; 61442-142; 68001-314; 68645-566; 70515-630; 70934-658; 71205-994; 57885-0008; 0093-0926; 51407-252; 53002-5700; 63629-1464; 68788-8326; 50090-0761; 70518-2727; 70934-415; 71205-993; 51846-1040; 73309-139; 82891-007; 55289-692; 61442-143; 61919-311; 68001-316; 68071-3261; 68071-4271; 68180-467; 68788-8287; 70518-3064; 71335-0882; 71610-709; 51927-5161; 58623-0021; 0093-0576; 51655-686; 63187-090; 63187-765; 68788-9668; 70518-2009; 71335-0819; 20076-0402; 68254-0001; 71052-668; 43063-983; 51407-253 |
| UNII |
9LHU78OQFD
|
| Synonyms |
Lovastatin | Mevinolin | Monacolin K | 6-Methylcompactin | 6 Methylcompactin | MK-803 | MK 803 | MK803 | Mevacor | Lovastatin, (1 alpha(S*))-Isomer | Lovastatin, 1 alpha-Isomer | 1 alpha-Isomer Lovastatin | Lovastatin, 1 alpha Isomer | alpha-Isomer Lovastatin, 1 |
|